Facial Pain and Headache
Pain syndromes of the face and head can be incredibly disabling. The head and face surround and protect our brains. The majority of our sensory input comes by way of sights, sounds, and smells. When patients suffer from facial pain or headache, every aspect of their lives can be affected, from sleeping to eating, brushing teeth to simply walking on a windy day. Trigeminal neuralgia and chronic migraine are two of the most common face and head pain syndromes, and both are often alleviated with surgical decompression of the nerves of the head and face.
Trigeminal Neuralgia
Trigeminal neuralgia (TN) is one of the most common facial pain syndromes in the United States. It is characterized by repeated, intermittent attacks of terrible, shooting pain in the distribution of the trigeminal nerve.
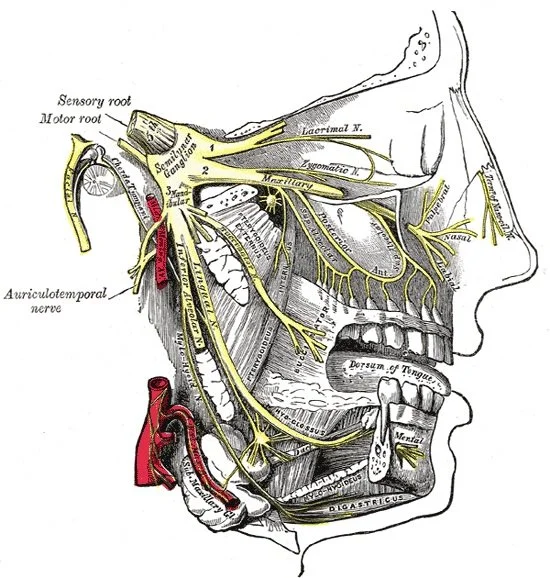
A drawing of the trigeminal nerve, showing its three distributions.
The pain due to TN can occur in any of the three distributions of the trigeminal nerve. Pain shooting down the cheek into the lower jaw is due to involvement of the mandibular nerve, or V3. Irritation of the maxillary nerve, or V2, causes pain through the cheekbone and into the upper lips and teeth. And pain in the ophthalmic nerve, or V1, distribution, causes pain in the eyes and forehead.
TN can have multiple different causes. The most common cause is compression of the nerve by a brain artery deep within the skull. The repeated pulsations of the artery cause pain to shoot down the rest of the nerve and be felt in the face, jaw, or teeth. Episodes of pain are often caused by mechanical irritation - often something as simple as eating, brushing teeth, or stroking the face.
When it is first diagnosed, patients with TN are started on medications such as carbamazepine (Tegretol) or gabapentin (Neurontin). Many patients experience excellent control of symptoms initially, but over time, the effectiveness of the medications can fade and pain attacks can return. Once medical treatment has failed, surgical procedures can be used to control the pain with excellent results. Dr. Hatef believes it is never too early to speak with a neurosurgeon about your options for TN and welcomes any patients to make an appointment.
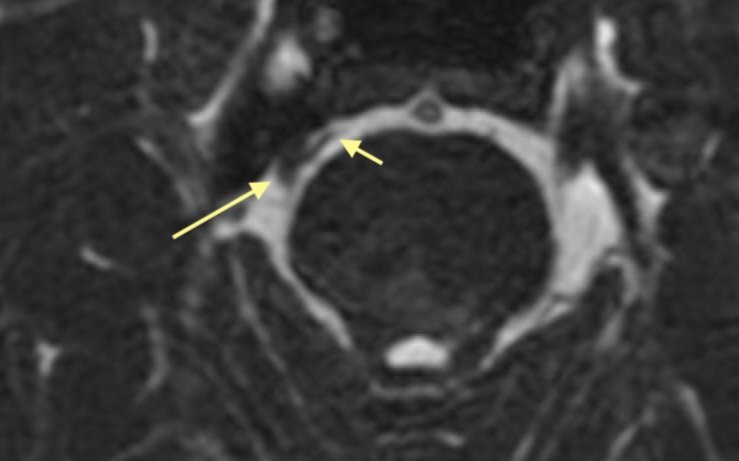
A cerebellar artery (short arrow) is compressing the trigeminal nerve (long arrow). This patient improved dramatically after decompression.
Options for surgery in trigeminal neuralgia depend greatly on the patient’s age, health, and wishes. For patients who have never been treated who are willing to undergo a craniotomy procedure, microvascular decompression (MVD) is considered the gold standard for pain relief. Dr. Hatef makes a small incision behind the ear and a small window in the skull to access the trigeminal nerve as it leaves the brainstem. The blood vessels that are compressing the artery are gently moved out of the way and a small cushion is placed to prevent re-compression. After just 1 or 2 days in the hospital patients return home, and can return to normal activity by 4-5 weeks.
For patients who do not wish to undergo a cranial procedure, there are two additional options. Some patients choose radiation therapy with stereotactic radiosurgery. Focused beams of radiation are used to damage the pain fibers of the trigeminal nerve while preserving those that give sensation to the face, decreasing pain.

Microvascular is a delicate microsurgical procedure performed to decompress the trigeminal nerve.
For those patients that have recurrent symptoms after an initial operation, or those that have medical problems and would prefer to avoid an invasive surgery, a procedure called rhizotomy is an option. Using only sedation, Dr. Hatef placed a small needle into the trigeminal nerve. He then stimulates gently to ensure the needle is in the correct place. With the needle correctly positioned, Dr. Hatef applies enough heat to damage the pain fibers while preserving sensation fibers. This results in a rapid relief of pain for most patients. This is a same-day surgery that even very frail patients tolerate well, offering pain relief for some of the most difficult cases.
Trigeminal neuralgia is a disabling disease with a multitude of treatment options. If you are suffering, Dr. Hatef promises to take the time needed to properly diagnose and counsel you regarding your symptoms.
Migraine
Migraine is a significant source of pain and disability in America. Migraines are often typified by throbbing, pulsating pain on one side of the head. Recently, more evidence has emerged that migraines are due to complex interactions between the nerves of the face and neck and the blood vessels surrounding them. Surgical decompression of these nerves can often alleviate pain.
Migraines originating from different nerves can cause different headache patterns. Involvement of the greater occipital nerve or lesser occipital nerve cause migraines in the back of the head and base of the skull. These can often be mistaken as originating in the cervical spine and are sometimes caused occipital neuralgia. Migraines over the temporal region are caused by compression of the auriculotemporal nerves, while those over the eyes and forehead are caused by compression of the supraorabital nerve bundle directly under the eyebrow. The surgical approaches to each nerve differ, and making the correct diagnosis is critical. Dr. Hatef works closely with a team of neurologists to correctly diagnose chronic migraines and ensure the correct nerves are decompressed.
Migraines can be caused by compression of the scalp arteries of the temple or eyebrow region.
The occipital nerves can be compressed by muscles or arteries in the neck and base of skull.